|
АкушерствоАнатомияАнестезиологияВакцинопрофилактикаВалеологияВетеринарияГигиенаЗаболеванияИммунологияКардиологияНеврологияНефрологияОнкологияОториноларингологияОфтальмологияПаразитологияПедиатрияПервая помощьПсихиатрияПульмонологияРеанимацияРевматологияСтоматологияТерапияТоксикологияТравматологияУрологияФармакологияФармацевтикаФизиотерапияФтизиатрияХирургияЭндокринологияЭпидемиология |
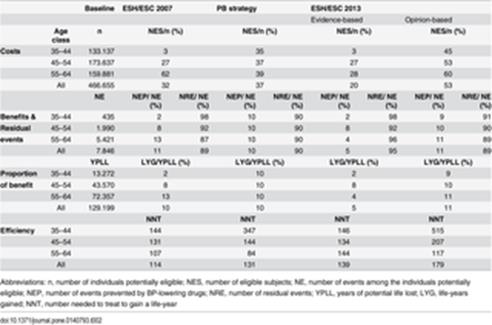
Sensitivity analysis. The 2013 guidelines approach indicates that treatment is recommended if evidence is available and it may or should be considered when evidence is weak or
The 2013 guidelines approach indicates that treatment is recommended if evidence is available and it may or should be considered when evidence is weak or unavailable. This is the case of grade 1 hypertension elderly patients and grade 1 hypertensives at low risk. We performed a sensitivity analysis to test to what extent the new recommendations could modify the proportions treated and benefits across the different categories of the potentially eligible population compared with the previous guideline version of 2007. We simulated the implementation of the new rule and assessed its impact on the NES and NEP, the number of residual events, i.e. the events that remained untreated in the individuals considered ineligible plus the events that remained despite BP lowering in treated individuals, the proportion of benefit and the efficiency. Elderly patients were identified as 60-year-olds and older individuals[24]. Ethics Statement Not applicable. Results The 2007 ESH/ESC guidelines provided 13074 life-years gained (NEP = 883) over 129199 years of potential life lost among the individuals potentially eligible (n = 466655), with a global proportional benefit coefficient of 10% (Table 2). The PB strategy resulted in a gender- and age-related gradient of risk-decision thresholds, with the highest threshold among individuals younger than 45 years and the lowest threshold in individuals over 55 years. While the proportions eligible to treatment showed a strong gradient related to age for both genders under the ESH/ESC strategy, this pattern was importantly attenuated in men and women by the PB strategy, with increased rates of treatment eligibility among individuals less than 55 (Fig 3). This implied an overall greater proportion of treated-to-untreated individuals under the PB strategy compared with the ESH/ESC strategy (37% versus 32% of the individuals potentially eligible on treatment, respectively).
Дата добавления: 2015-11-26 | Просмотры: 522 | Нарушение авторских прав |