|
АкушерствоАнатомияАнестезиологияВакцинопрофилактикаВалеологияВетеринарияГигиенаЗаболеванияИммунологияКардиологияНеврологияНефрологияОнкологияОториноларингологияОфтальмологияПаразитологияПедиатрияПервая помощьПсихиатрияПульмонологияРеанимацияРевматологияСтоматологияТерапияТоксикологияТравматологияУрологияФармакологияФармацевтикаФизиотерапияФтизиатрияХирургияЭндокринологияЭпидемиология |
Physiology of respirationRespiration is divided into external and internal. External respiration ensures a supply of oxygen (02) from the atmosphere to the blood of pulmonary capillaries and carbon dioxide (C02) release from it into the atmosphere. Internal respiration includes transport of blood gases and tissue respiration. Proceeding from this a respiratory system fulfils the following basic and nonrespiratory functions: 1. Ensures metabolism by means of supplying necessary amount of oxygen to the tissues and removal of carbon dioxide from the tissues. 2. Metabolic function: "biochemical filtration" of biologically active substances (BAS) is provided by endothelial and neuroendocrine cells (Fetter's and Kulchitsky's cells, cells of APUD-system), as well as a complete set of enzymatic systems of detoxication (oxidation, methylation and others). 3. Metabolic control over local and systemic hemodynamics by means of synthesis, deposition, activation and degradation of BAS (angiotensin-converting enzyme, norepinephrine, serotonin, prostaglandins, etc.). 4. Metabolic control over a system of homeostasis. Enzymes, receptors, inhibitors and activators of the factors of homeostasis system are revealed in the endothelium of vessels of pulmonary microcirculation. 5. Participation in water-salt metabolism and heat exchange. About 700 ml of liquid are released from the lungs by perspiration daily. The difference between oncotic (25 mm Hg) and hydrostatic (8-10 mm Hg) pressure ensures a rapid absorption of liquid by a pulmonary blood flow (this feature is used for endotracheal administration of drugs in cardiopulmonary resuscitation). 6. Provision of immunologic response (there is a high level of lysosomic enzymes of leukocytic origin in the blood outflowing from the lungs). 7. Retention of mechanical and infectious bodies, as well as toxic substances that get from the atmosphere (this is ensured owing to mucociliary clearance and cough reflex). 8. Participation in the metabolism of proteins and fats at the expense of lipolytic and proteolytic enzymes. A synthesis of surfactant (by the 2-nd order alveolocytcs) that ensures an optimal level of alveolar surface tension.
A disturbance of pulmonary metabolic function occurs in the most different forms of pulmonary pathology, as well as in the disorder of systemic hemodynamics (shock), when a "metabolic load" upon the lungs increases. 1. Central regulator. There is a medullar respiratory center in the reticular A center of pneumotaxis is arranged in the upper sections of pons varolii. It limits the length of inhalation exerting so its effect on the respiratory rate. There is an apneastic center located in the lower part of pons varolii. When regulation of the respiratory function is switched over to this section an apneastic respiration (agonal state) appears. Hypothalamus and limbic system also have their own independent inspiratory activity. 2. Effectors: diaphragm, intercostal musculature, muscles of the abdominal wall and auxiliary musculature. 3. Receptors that take part in reflex regulation of respiration arc located in the lungs, vessels and the brain. Central chemorcceptors arc located on the ventral surface of medulla oblongata near the outlet of the IX and X pairs of cranial nerves. The principle stimulus of these receptors is the concentration of H+ and PCO, in the cerebrospinal fluid (CSF). A decrease of CSF pH contributes to the increase of ventilation (Kussmaul respiration in ketoacidosis, hyperventilation syndrome in grave craniocerebral injury) and vice versa. Peripheral chemorcceptors (carotid and aortic bodies) react to the change of gas composition of blood. An increase of pulmonary ventilation (high altitude sickness) occurs when Pa 02 decreases (lower than 80 mm Hg) and Pa C02 elevates. Stretch receptors of the lungs respond to the increase of lung volume owing to which the inhibition of inspiration occurs. The irritant and juxtacapillary receptors are also located in the airways. Mechanics of respiration I. Conductive zone of the lungs (trachea and bronchi): 0-16 order. Anatomically dead space (150-175 ml). II. Transitional (transitory) zone (respiratory bronchioles of the 1-3 order): 17-19 order. A minimal gas exchange starts in this zone. III. Respiratory zone (acinus) — 20-23 order. A gas exchange takes place A transfer of air from the external medium to the alveoli occurs due to the difference of pressures between them. During inspiration a negative pressure (-30 mm water column) is formed in the airways. Expiration is a passive process and occurs at the expense of elastic forces and alveolar surface tension. In the beginning of expiration the pressure becomes positive (3 cm water column) in the respiratory tracts. Mainly, the resistance of two types counteracts a transfer of air into the alveoli:
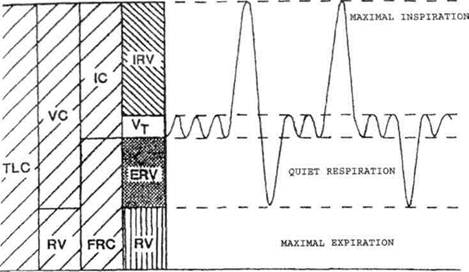
Total compliance decreases with age, in thorax deformation, atelectasis, pneumonia, pulmonary edema and limitation of diaphragm mobility. 2. Nonelastic resistance — it is a resistance to respiration arising in movement of air along the respiratory tracts as a result of friction of air particles against the walls of respiratory tracts. In bronchial asthma it increases 10-30 times, and owing to this a percentage of oxygen consumption by respiratory muscles increases (up to 50%). Opioids are also able to cause a rigidity of the chest, thereby impeding the adequate ventilation. An important role in the formation of elastic resistance is played by surfactant (Clement's factor) — phospholipid changing the strength of surface tension. The main role of surfactant system of the lungs is to prevent alveoli collapse, decrease of transpulmonary pressure and muscular efforts in inspiration. In case of surfactant defficiency RDS and atelectasis develop. Hypothermia, disturbance of nourishment of the alveolar tissue and others contribute to a decrease of surfactant level. Ventilation. It is characterized by a number of volumes and capacities originating from them (Fig. 27).
Дата добавления: 2015-02-05 | Просмотры: 1194 | Нарушение авторских прав |